Distinguishing the Community Health Model
The community health model differs from both law and medicine. Unlike law and medicine, community health's primary focus is neither the individual nor an individual's rights or interest. Community health policy is concerned with protecting the public—the community as a whole. Except to the extent that improving individual health improves the community health, its primary concern is not individual health. A community functions only as well as the members of the community are healthy. Thus, the goal of community health is to assure optimal health for all its individual members.
Since communities differ greatly, promoting the community's health has to be done within the context of the community's need. Just as Maslow defined the needs for individuals, every community has a sociological explanation of it needs and consequently its behavior.' Every community has several levels of needs:
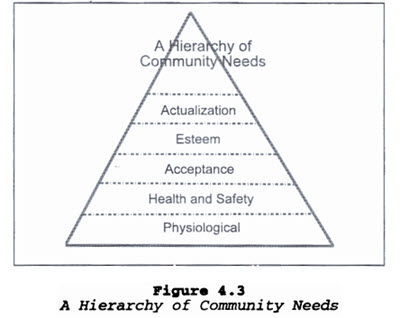 Physiological Needs: This first level of community motivators includes such needs as hunger, clothing and personal comfort.
Physiological Needs: This first level of community motivators includes such needs as hunger, clothing and personal comfort.
Health and Safety Needs: This second level of community motivators includes health, security, protection, freedom from fear, anxiety and chaos, need for structure, order, law.
Acceptance Needs: This third level includes the need for the community to be accepted and to be recognized by the society at large.
Esteem Needs: The fourth level of the hierarchy focuses on the need for the community to be respected by others and to attain self-confidence, strength, a feeling of worth.
Community Actualization Needs: The fifth level of the hierarchy represents the highest level of fulfillment that communities can strive for; communities that reach actualization realize their full potential.' (See Figure 4.3).
In accordance with Maslow's theory, as individuals satisfy their own needs and come closer to actualizing their innermost potentials, they become increasingly devoted to the happiness of others. Self-actualized people use their potentialities for creative results that are beneficial to themselves and to society as a whole; they surmount the dichotomy between individual development and the common good. However, the functional level of a community is based on the resources needed to address an individual's basic needs. Thus, a minority of individuals in a community can determine the functional level of the community if that minority represents a significant portion of the community. Essentially, the functional level of a community is based on the lowest level of need that a significant portion of the community is still struggling to meet.
Thus, where a significant portion of a community is still struggling to meet their need for food, shelter, and clothing (i.e., the homeless community), the functional level of the community is at the physiological level. Similarly, where a significant portion of the community is struggling with issues of violence, drugs, illness, and death (i.e., inner city communities), the functional level of the community is at the safety and health level.
Community needs are hierarchical and the community's pursuit of a higher need is impaired until a lower need is substantially met. However, once lower needs are met, it is the higher unmet need that becomes the basis for motivation. Thus, identifying and helping a community to meet its unmet needs is essential not only to the survival of the community but to its growth and development as well.
The ultimate need that every individual has, and thus every community, is "actualization." Community actualization is the community's efforts to maximize its talents and resources--its effort to become all that it can. However, a community can't focus on actualization if its needs for food, clothing, shelter, safety, or health are not met. Rather, communities, like individuals, will focus on obtaining "lesser" unmet needs. Consequently, the focus of community health should be to see that the basic community need, a satisfactory level of health, is met. No community can become actualizing without health.
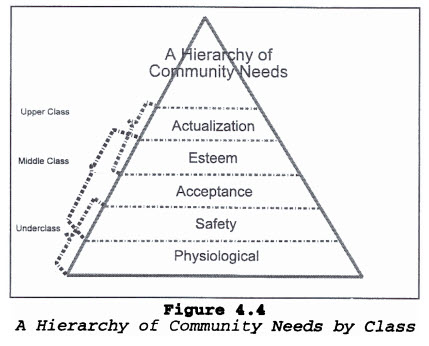 In a class-based society, we have communities that are functioning and competing on different need attainment levels. Many middle-class and upper-class communities' unmet needs are esteem and actualization. Individual rights and interests are necessary for individuals to become self-actualized and to develop strong esteem. Consequently, individual rights are also necessary for a community that is working to develop esteem and to become actualized. Thus, for many middle- and upper-class communities, protecting individual rights and interests is a prerequisite for their community's need fulfillment.
In a class-based society, we have communities that are functioning and competing on different need attainment levels. Many middle-class and upper-class communities' unmet needs are esteem and actualization. Individual rights and interests are necessary for individuals to become self-actualized and to develop strong esteem. Consequently, individual rights are also necessary for a community that is working to develop esteem and to become actualized. Thus, for many middle- and upper-class communities, protecting individual rights and interests is a prerequisite for their community's need fulfillment.
Underclass communities struggling to obtain food, clothing, housing, safety, and health and middle-class communities struggling to obtain acceptance may view the rights and interests arguments advanced by those seeking esteem and actualization of lesser importance. This is a very significant fact when considering the impact needs fulfillment has had on policy-making in medicine, law, and community health. Since most of the policy makers and providers are functioning at least at a middle-class needs level, and many of their communities are striving to become actualized, much of the discussion around problem-solving is centered on protecting rights or interests. The result is that the policy makers and providers filter the potential policy, law, or intervention through their own community need for esteem and actualization.
Certainly, individual rights and interests are important to all communities, but they should not be the primary focus for basic community health policy. It may be an appropriate part of the legal analysis and it is certainly an appropriate part of the political analysis, but the discussion must also include a community needs focus.
Of course, a major question becomes how will that community focus be actualized without infringing on individual rights? Frankly, as long as we continue to think of individual rights and community interests as dichotomous needs in conflict with each other, it is impossible to construct a solution. Community Health Interventions
To that end, then, we can now look at the traditional public health approach to promoting community health. Public health interventions can be classified as primary, secondary, and tertiary intervention. Primary intervention steps in and prevents disease entirely--the disease never happens and never occurs. For example, school vaccination, fluoridation of the community water, and sanitation efforts are all primary community health interventions.
Tertiary interventions are efforts to minimize the long-term effect of a disease. Tertiary intervention is not prevention. The disease or disorder has occurred; effort is directed at minimizing the effect. Tertiary intervention is treatment. The baby is here, we cannot stop fetal alcohol syndrome, how do we now deal with it, how do we now help that child affected by fetal alcohol syndrome? It is treating a problem that has not been prevented--a problem that exists because primary and secondary interventions were not effective. For example, diet and exercise will not prevent diabetes. Rather, these interventions will affect the impact of the disease on the individual and thus the community.
Many people tend to think of community health as prevention. But prevention is only one aspect. Treatment is an aspect since the community is just as affected by the diseases that go untreated as by those that go unprevented. So, though we can't prevent a disease, it is nevertheless appropriate to implement tertiary community health intervention.
Secondary interventions fall between prevention and treatment. These efforts are both to prevent the further development of the disease and to lessen the impact of the existing disease. For example, throat cancer is fairly curable if caught early.